Dear Mr. Huxley…
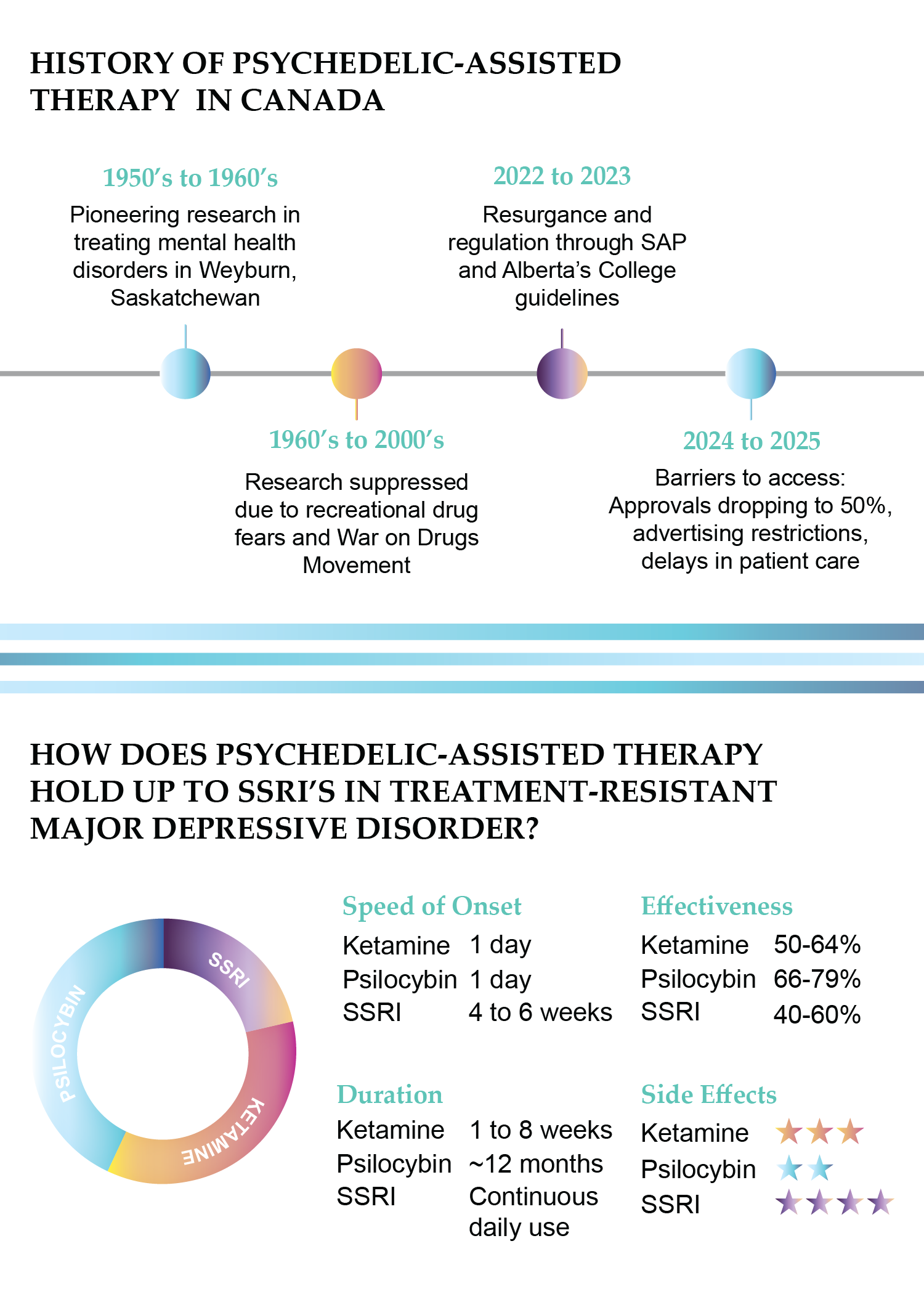
It was an unusually mild winter for Saskatchewan in March 1956, and the halls of Weyburn Mental Hospital, a facility renowned for some of the most cutting-edge, experimental treatments of its time, fell silent for the evening.
Weyburn clinical director and researcher Humphry Osmond had spent the day immersed in groundbreaking trials, exploring the effects of mescaline and LSD (Lysergic Acid Diethylamide) on patients with schizophrenia and those hospitalized for delirium tremens – a severe, late-stage alcoholism disorder causing hallucinations, similar to schizophrenia.
During his time at Weyburn, Osmond began to write what became a series of letters with his dearest friend and confidant, novelist Aldous Huxley, author of A Brave New World. discussing his progress in the field of psychedelic psychiatry.
In these handwritten letters, somewhere between bonding over a mutual distaste for the original term, psychotomimetic, meaning “to divide the mind”, and Huxley’s deep passion for etymology, the duo coined the now widely adopted term psychedelic, tracing it back to Greek and Latin roots meaning “expansion of the mind.”

Osmond’s clinical trials would later show that LSD eliminated cravings in 40 to 45 per cent of more than 2,000 patients hospitalized for late-stage alcoholism. These patients maintained sobriety after one year of the trial. To this day, this achievement remains significant in addiction treatment.
Despite the study’s success, Osmond’s research was banned in the 1960s amidst growing concern around recreational drugs in the lead-up to the War on Drugs movement. Osmond passed away in 2004, but his research has resurfaced in recent years with the resurgence of interest in psychedelic-assisted therapy.
In early January, 2022, amendments were made to a federal emergency medical pathway called Canada’s Special Access Program (SAP), allowing physicians to request psychedelics for those suffering with treatment-resistant mental illness.
Leading the charge in this new wave of medicine was Alberta, setting regulatory guidelines for psychedelic-assisted therapy in 2023, paving the way for the rest of Canada. It was starting to look as though Osmond’s pioneering research was finally going to see the light of day.
Over the past year, however, psychedelic-assisted therapy professionals across Canada have faced increasing delays to client care, citing 15-page rejection letters from Health Canada, and stricter advertising laws targeting clinics that have existed for years without incident – some letters even involving RCMP.
The question is no longer whether these treatments work, it is whether they will survive Canada’s increasingly restrictive health system while other countries are rapidly progressing in access to this type of care.
So, is the clinical use of psychedelics in Canada becoming uprooted before it has a chance to grow?
Brenda’s story
Several decades after Dr. Osmond’s research was shut down, Brenda Colene Goodbody stepped off the plane in Saskatchewan for her first intravenous ketamine infusion. She had never tried recreational drugs. Now, standing outside the ketamine clinic, she froze.
She called her therapist, “I can’t do this. Maybe I’m just making it up, maybe there’s nothing wrong with me.”
Her therapist reminded her why she had sought out the referral. Goodbody has lived with severe depression and suicidal ideation since she was 13, cycling through more than a dozen antidepressants over the years without relief.
Multiple misdiagnoses had followed, before she was finally diagnosed with bipolar disorder. Her psychiatrist recommended lithium or topiramate, but after years of undesirable side effects from antidepressants, she did not want to risk the side effects of such heavy drugs.
Goodbody explains that with traditional methods, there is often a trial and error phase. It can take four to eight weeks to adapt to the medication, and if it fails, it can take another four to eight weeks to taper off that medication before starting a new one.
“We’re told to ‘take this pill and just get over it’, and if the pill doesn’t work, well, just try harder to get over it,” says Goodbody.
Some medications Goodbody was previously prescribed had warnings, white text in black boxes, printed on the orange pill bottles that read: this medication may cause suicidal thoughts, the very thing Goodbody was seeking treatment for.
“I can tell you with 100 per cent certainty that ketamine saved my life, and it didn’t just save it, but it gave me a life that I’ve never dreamt existed or was even possible. It’s such a shift from waking up, wishing you were dead, to actually feeling joy.”
When her doctor recommended lithium, she asked if she could try ketamine infusions instead. As a psychology student, she had spent long nights researching ketamine’s effect on treatment-resistant disorders, finding that it had a 50 per cent success rate. Her psychiatrist agreed she would be a suitable candidate for the treatment.
Taking this into account, Goodbody calmed her anxiety and walked inside the clinic.
She described the 60-minute ketamine infusions as deeply immersive, she felt as though she was having an out-of-body experience. During her session, she envisioned millions of tiny worker men with rucksacks and little axes, marching through her brain and repairing all her neurons.
“That vision always stuck with me,” says Goodbody. “Because that is exactly what the treatment is doing. It comes in, repairs neural connections, and creates new ones.”
Flying back to Calgary, Goodbody noticed a shift. Where she once felt numb, walking through life on autopilot, she was now waking up with joy and looking forward to taking walks through the park.
“I can tell you with 100 per cent certainty that ketamine saved my life, and it didn’t just save it, but it gave me a life that I’ve never dreamt existed or was even possible,” says Goodbody. “It’s such a shift from waking up, wishing you were dead, to actually feeling joy.”
Goodbody went on to complete her studies in psychology, writing her master’s thesis on the ethical considerations of providing Medical Assistance in Dying (MAiD) for mental illness, emphasizing how we have other treatment options, citing her own success story with ketamine infusions.
“It just feels so wrong,” she says. “It’s unethical to fund someone’s death but not their chance to live. I want to stress that it is not a cure, but we have treatment options that can help people. The government needs to step up and start funding them for the most severe cases.”
Goodbody is now a registered provisional psychologist, yet she was shocked to learn that she would need five more years of practice before she could put her experience to work within the field of psychedelic-assisted therapy.
While similar practices only require an extra 400-500 hours of supervised work in the field, there is not a set number of hours required for a psychologist to provide therapy in a psychedelic-assisted clinic.
Therapists determine the training and competency needed, which could range from a few weekend workshops to formal programs of 40-plus hours, depending on the modality and context.
Changing Behaviour
While Goodbody’s journey shows promising results for these treatments, her path also highlights broader regulatory hurdles that continue to slow down the industry nationwide.
Across the country, health professionals, psychologists, and therapists who have dedicated their lives and careers to advancing a promising revival of potentially life-saving treatment are now seeing door after door shut in their faces, often with little to no explanation.
On paper, the process looks fairly straightforward. Doctors can request restricted substances like psilocybin, more commonly known as magic mushrooms, for individual patients through SAP, while clinics and researchers can operate multi-patient programs, provide training, and conduct studies under what are known as Section 56 exemptions.
In practice, however, these two pathways have created more confusion than clarity. Case-by-case SAP exemptions have led to prolonged wait times for patient care amidst a nation-wide mental health crisis, while facilities who have spent years building safe, evidence-based programs now face longer delays and sudden rejections through Section 56 despite full compliance.
“For years, clinics offering ketamine therapy operated safely and transparently. Suddenly, we’re told that mentioning treatment options online could trigger enforcement. It’s confusing and discouraging. Clinics are doing everything by the book, yet the rules seem to be changing mid-stream.”
Liam Bedard, executive director of Ontario-based PsyCan, a not-for-profit trade association for Canadian psychedelic medicine and therapy companies, says his organization was recently hit with 15-page rejection letters from Health Canada.
Bedard states that since 2024, Health Canada’s approval process for Section 56 and SAP applications has slowed significantly, with clinics across the country seeing approval rates drop by close to 50 per cent compared to previous years.
Meanwhile, public opinion is moving in the opposite direction. A recent Abacus Data poll found that a majority of Canadians support the medically supervised use of natural psilocybin, with only one in four opposed.
“It’s like being stuck in the waiting room,” says Bedard. “It’s like hallway medicine. The SAP is the hallway medicine of mental health care.”
Even Alberta, praised for establishing clear regulatory pathways through its professional colleges, is also feeling the pressure.
In early 2023, The College of Physicians and Surgeons of Alberta, the College of Psychologists, and the College of Social Workers had all issued guidance allowing accredited clinics to operate legally, but federal responsiveness has slowed as of late, says Reverdi Darda, co-founder of psychedelic-assisted therapy clinic ATMA CENA, and chair of the Multidisciplinary Association of Psychedelic Studies (MAPS) Canada.
“Over the past six months, Health Canada’s behaviour has changed,” she explains. “We’re seeing new types of correspondence, more rejections, and compliance warnings we haven’t seen before.”
Just last month, a once hopeful Darda was surprised to find letters from Health Canada come across her desk regarding advertising compliance, some letters even involving the RCMP.
“For years, clinics offering ketamine therapy operated safely and transparently. Suddenly, we’re told that mentioning treatment options online could trigger enforcement.” says Darda. “It’s confusing and discouraging. Clinics are doing everything by the book, yet the rules seem to be changing mid-stream.”
While these changes in behaviour stir uncertainty in service providers who have dedicated their lives and careers to create a safer alternative to traditional treatment methods, many patients are facing prolonged wait times for what could be life-saving care.
“We are potentially doing more harm to our clients the longer these delays go on,” says Darda. “It’s heartbreaking to watch people lose hope while the paperwork sits.”
These frustrations extend to research and care for those who served in the military. In Ontario, PsyCan has been working to expand psychedelic-assisted therapy for Veterans Affairs Canada (VAC) but the initiative is trapped in a catch-22: VAC insists on stronger evidence before funding large-scale access, yet it has not approved the Senate-recommended federal research program required to produce that evidence.
The consequences are devastating. At a recent parliamentary press conference, Gordon Hurley, a former Canadian Special Operations Forces Command operator, declared that in the past two years, 280 veterans have died by suicide, equating to one veteran every three days.
“Texas just invested $150 million into ibogaine research for opioid use disorder and PTSD among veterans. How is one of the most conservative states in America light years ahead of our great nation of Canada that prides itself on our progressive nature and values?” Hurley asked in the press conference.
Just one year earlier, Kelsi Sheren, combat veteran, author, and life coach said she had to leave Canada to access the psychedelic-assisted therapy that saved her life. When she tried to receive treatment here, she was shocked to discover that Health Canada required her to undergo electroconvulsive therapy before even considering psychedelics, despite her having a traumatic brain injury.
“It’s time for a proper regulatory approach,” Darda says. “We already have evidence that these therapies work. What’s missing is the political will to make access safe, consistent, and compassionate.”
Allison’s story
“CPTSD? Isn’t that only something that war veterans get?” Allison Waylon felt as though she had to look over her shoulder to see who her psychiatrist was speaking to.
That couldn’t possibly apply to her, she thought to herself. On the other hand, she did seem to check all the boxes.
Still unsure, she sought out several other professionals before confirming the diagnosis for herself. Complex Post-Traumatic Stress Disorder, a condition plagued by flashbacks of multiple traumatic events, nightmares, a constant undercurrent of anxiety, and feeling detached from oneself.
Waylon carried deep wounds from prolonged and repeated trauma for so long over the course of her life that emotional overwhelm felt normal to her, shaping her identity around lack of safety and self-worth. Yet, she pushed through, wearing her resilience like a badge of honour.

PHOTO: HEATHER JOHNSTON
Even so, lately the pressure had been getting to her. She had just turned 50 when she discovered her husband had been diagnosed with stage 4 metastatic melanoma. She tried to stay strong as she had for so many years, but her emotional armor started to crack under the weight of a nervous system pushed past its limits.
Swallowing her pride, she booked the appointment to speak with a psychiatrist.
“Are you hypervigilant?” her psychiatrist asked.
“Well, yeah. Isn’t everybody?” she replied.
Waylon thought back to all the times she felt anxious, when others seemed to be able to brush it off. She had been experiencing sleepless nights for weeks and flashbacks to traumatic events of her past.
Waylon had already tried every traditional therapy method she could think of. Support groups, mindfulness, experiential workshops. All helped in important ways, but she found they only helped her to cope and did not truly heal her. She had been on medication on and off since she was a teenager, but she never found that it did much of anything.
With her husband’s condition worsening, she began looking into psychedelic-assisted therapy end-of-life care. After researching the treatment extensively, the Waylons discovered that psilocybin had phenomenal results in military veterans suffering from the same condition that was severely impacting Allison’s daily life.
Like Goodbody, Waylon had never tried recreational drugs and rarely drank alcohol. When her spouse dropped her off at the Calgary-based clinic, she was filled with a mix of nerves and cautious hope. She was the first person to receive treatment at the new facility.
Friendly staff greeted her in a room that glowed in soft lighting, furnished with comfy couches, pillows, and weighted blankets. Before they began, her therapist revisited her intentions: what she was hoping to achieve, what fears she carried, and what safety anchors she could hold on to if she felt overwhelmed at any time–reminding her that she would not be alone.
“For someone so used to carrying that fear in silence, that reassurance was the beginning of the healing process,” Waylon says.
When it was time, she was given the psilocybin dose and laid down in a reclining chair, covering her eyes with light-blocking eye shades. She was given headphones with carefully chosen frequency music guiding her emotional flow throughout the process.

PHOTO: ATMA CENA
When her nervous system wanted to kick up a notch, and the medicine opened a door to a memory or emotion she normally could not touch without shutting down, she found that this time, it did not crush her. “Something shifted. It moved like a story across a video screen, and I was able to finally witness it with compassion,” says Waylon.
At the end of the session, she regrouped with the team, and they made sure she was grounded before they knew she was safe to go home.
Later, at her place, Waylon started feeling subtle yet profound effects. Her nervous system calmed down, anxiety reduced, and she started to realize she had an improved social connection.
Her friend’s birthday was coming up, which would typically put her in a spiral of social anxiety. This time though, her husband was surprised to see that she was excited to give her friend a call and take her out for dinner.
Though Waylon is still early in her treatment, she stresses it has transformed her life in ways that traditional methods never did.
“The support I received unlocked doors for me that had been locked for a very long time. I saw my trauma through new eyes,” says Waylon. “They helped me find light in places I thought would always stay dark. Their presence, skill, and compassion made my journey easier.”
Root Resistance
Canada has a deeply rooted history in psychedelic-assisted therapy research, pioneering studies by Humphry Osmond and others as early as the 1950s and 1960s. Nevertheless, it is quickly falling behind other G7 countries like the United States and Australia, which are moving quickly to establish regulatory frameworks for psychedelic-assisted therapy, a treatment that many are calling life-saving care.
Without decisive action, the lives of those transformed by psychedelic-assisted therapy risk an inability to access care, while Canada risks both its pioneering legacy and the opportunity to reshape a mental health care system that many already struggle to navigate.